Proximal Row Carpectomy (PRC) is a surgical procedure performed to treat certain wrist conditions that cause pain, stiffness, and loss of function. It involves the removal of the proximal row of carpal bones—the scaphoid, lunate, and triquetrum—to relieve symptoms and preserve wrist motion. PRC is considered a motion-preserving salvage procedure and is often an alternative to wrist fusion in selected patients.
The wrist is a complex joint composed of eight small carpal bones arranged in two rows: the proximal row and the distal row. The proximal row consists of the scaphoid, lunate, triquetrum, and pisiform bones. These bones articulate with the radius and ulna proximally and the distal carpal row distally, allowing for a wide range of wrist motion including flexion, extension, radial and ulnar deviation.
The proximal row plays a critical role in wrist stability and load transmission. However, when these bones are damaged due to trauma, arthritis, or avascular necrosis, they can become a source of pain and dysfunction.
PRC is primarily indicated in patients with:
Patients selected for PRC typically have preserved cartilage on the capitate and radius, as the procedure relies on the articulation between these two surfaces after removal of the proximal row.
Before surgery, detailed imaging studies such as X-rays, CT scans, or MRI are performed to assess the extent of arthritis and cartilage condition. The surgeon evaluates the integrity of the distal carpal row and the radius to ensure suitability for PRC.
Anesthesia and Positioning: The procedure is usually performed under general or regional anesthesia with the patient’s arm on an arm table.
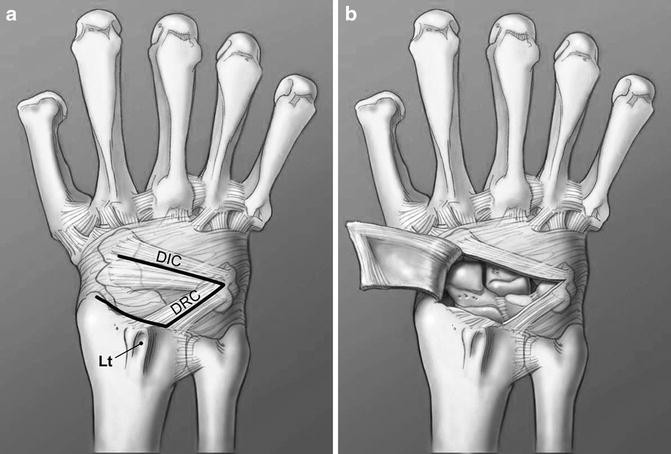
Incision: A dorsal longitudinal or curvilinear incision is made over the wrist to expose the carpal bones.
Exposure: The extensor retinaculum and dorsal wrist capsule are carefully incised to access the proximal carpal row.
Removal of Proximal Row: The scaphoid, lunate, and triquetrum are excised en bloc. Care is taken to preserve the cartilage on the distal radius and capitate.
Assessment of Articulation: The surgeon inspects the capitate and radius surfaces to confirm they are suitable for articulation.
Closure: The capsule and retinaculum are repaired, and the skin is closed in layers.
Immobilization: The wrist is immobilized in a splint or cast postoperatively.
After surgery, the wrist is immobilized for approximately 4 to 6 weeks to allow soft tissue healing. Early motion exercises are then initiated under the guidance of a hand therapist to restore range of motion and strength.
Rehabilitation focuses on:
Patients typically regain a functional range of motion, although some loss compared to the normal wrist is expected.
Proximal Row Carpectomy offers several advantages:
Studies have shown that PRC provides good to excellent outcomes in carefully selected patients, with pain relief and functional improvement lasting for many years.
PRC is not suitable for all patients. Contraindications include:
In such cases, alternative procedures like partial wrist fusion or total wrist arthrodesis may be considered.
As with any surgery, PRC carries risks, including:
Close follow-up and adherence to rehabilitation protocols help minimize complications.
PRC is often compared with four-corner fusion (4CF), another motion-preserving salvage procedure. While 4CF fuses the capitate, lunate, hamate, and triquetrum bones, PRC removes the entire proximal row. PRC generally allows for greater wrist motion but may have a higher risk of progressive arthritis. The choice depends on patient factors, surgeon preference, and specific pathology.
Proximal Row Carpectomy is a valuable surgical option for patients with certain types of wrist arthritis and carpal bone pathology. By removing the diseased proximal carpal row, PRC alleviates pain while preserving wrist motion and function. Proper patient selection, meticulous surgical technique, and dedicated rehabilitation are essential for optimal outcomes. Patients considering PRC should discuss the benefits, risks, and alternatives with their orthopedic surgeon to make an informed decision.
Chat With Me